

Action Alert
AHA Comment Letter on Hyberbaric Oxygen Therapy Rate in CMS' OPPS CY 2024 Final Rule
The Honorable Chiquita Brooks-LaSure
Administrator
Centers for Medicare & Medicaid Services
Hubert H. Humphrey Building 200
Independence Avenue, S.W., Room 445-G
Washington, DC 20201
Re: CMS–1786–FC: Medicare Program: Hospital Outpatient Prospective Payment Final Rule (Vol. 88, No. 224), November 22, 2023.
Dear Administrator Brooks-LaSure:
On behalf of our nearly 5,000 member hospitals, health systems and other health care organizations, and our clinician partners — including more than 270,000 affiliated physicians, 2 million nurses and other caregivers — and the 43,000 health care leaders who belong to our professional membership groups, the American Hospital Association (AHA) is writing to express concern about a reduction of over 40% in reimbursement for hyperbaric oxygen therapy (HBOT) that was published in the Centers for Medicare & Medicaid Services’ (CMS) hospital outpatient prospective payment system (OPPS) final rule for calendar year (CY) 2024. Our analysis of the OPPS data shows that the final rule rate for this service is erroneous; therefore, we urge CMS to issue a notice correcting it prior to Jan. 1, 2024.
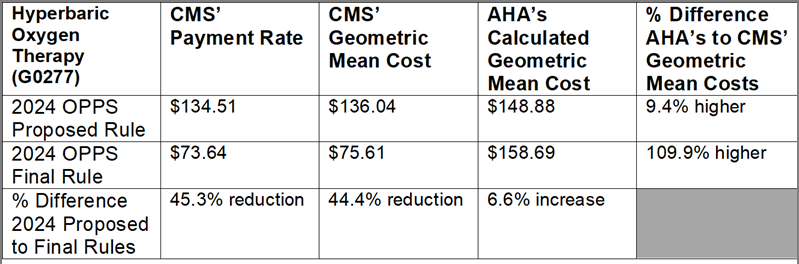
In the CY 2024 OPPS proposed rule, CMS proposed a payment of $134.51 for HBOT, a 7.5% increase from the CY 2023 rate. However, the final rule’s published payment was only $73.64, a 45.3% reduction from the proposed rule. Neither the proposed nor final rule discussed any change in policy for this service and there are no obvious reasons for such a substantial change between the proposed and final rules.
That said, the AHA nevertheless analyzed the CY 2024 proposed and final OPPS rate-setting data to try to determine the source of the change. We created a subset of claims with Healthcare Common Procedure Coding System code G0277 (HBOT), and then attempted to replicate the CMS value using the current methodology for HBOT, as we understand it, as well as by changing the current methodology in various ways. Our analysis found claim counts for HBOT similar to CMS’ claim counts. It also yielded a geometric mean cost for HBOT (based upon proposed rule data) that was slightly higher than CMS’ but in the same ballpark (see the table below). However, the geometric mean cost we calculated based upon final rule data ($158.69) was substantially higher — nearly 110% more — than CMS’ geometric mean cost ($75.61). As noted, AHA made various adjustments to the methodology to see if we could understand what might have made CMS’ own value drop significantly between the proposed and final rules. However, nothing we did was able to explain the substantial difference between CMS’ and AHA’s calculations.
A cut of this magnitude would devastate patient access to HBOT across the country, putting vulnerable patients at risk. In addition, this reduction would have a consequential effect on access to critical associated services that depend on HBOT, including wound care. HBOT is a proven therapy that exposes a patient to pure oxygen in a pressurized environment to promote wound healing, saves limbs from amputation and reduces the risk of death for conditions such as acute carbon monoxide intoxication, decompression illness, crush injuries and diabetic wounds of the lower extremities. It is a critical treatment option in advanced wound care and has improved and maintained quality of life for hundreds of thousands of patients.
We can only conclude that CMS made an error in its CY 2024 final rule rate. Therefore, the AHA urges the agency to reevaluate its calculations of the HBOT rate and issue a correction that establishes an accurate payment. We presume such a rate would be closer to the $158.69 figure that the AHA calculated.
We appreciate your consideration of these issues. Please contact me if you have questions or feel free to have a member of your team contact Roslyne Schulman, AHA’s director for policy, at rschulman@aha.org.
Sincerely,
/s/
Ashley Thompson
Senior Vice President, Public Policy
Key Resources
Related Resources
Guides/Reports
Guides/Reports