

Letter/Comment
Estimate of Federal Payment Reductions to Hospitals Following the ACA 2010-2026: Estimates and Methodology
Table of Contents
Medicare Payments for Bad Debt ...........................................................3
Reduction in Post-Acute Care (PAC) Provider Payment Updates............3
Hospital Coding and Documentation Adjustments .................................4
Adjustment to Inpatient Hospital Payment Rates...................................4
Provider-Based Off-Campus Hospital Outpatient Departments..............5
Medicare Payments for Long Term Care Hospitals ................................5
Clarification of 3-Day Payment Window .................................................5
Total Impact of Reductions on Federal Payments to Hospitals ..............6
Executive Summary
Dobson DaVanzo & Associates was commissioned by the Federation of American Hospitals (FAH) and the American Hospital Association (AHA) to estimate the cumulative federal payment reductions to hospitals from 2010 through 2026 in addition to those that were enacted under the Affordable Care Act (ACA).1 Nine legislative Acts were identified as well as regulatory changes by the Centers for Medicare and Medicaid Services (CMS) that are estimated to reduce federal payments to hospitals by $148.75 billion over this period. Exhibit ES-1 shows the level of reductions by type.
Exhibit ES-1: Federal Payment Reductions to Hospitals 2010-2026 In Addition to ACA (in billions)
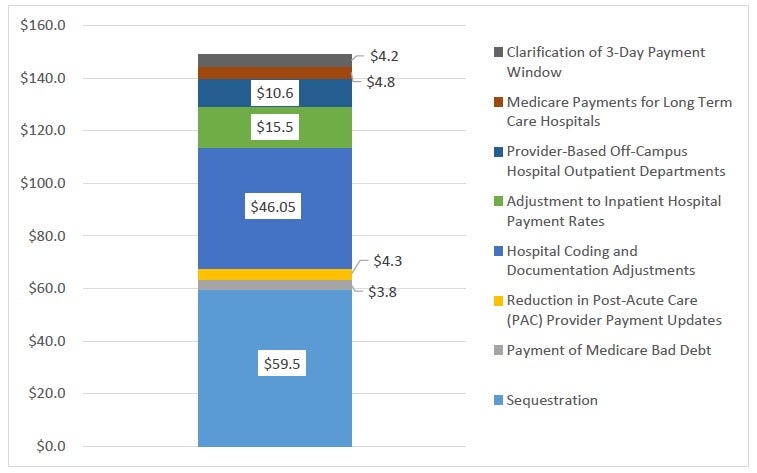
Source: Dobson|DaVanzo estimates – sources and methodology described below.
The following sections describe the sources for each of these federal payment reductions.
1. For this analysis, we included acute care (inpatient and outpatient services), free-standing inpatient rehabilitation, long-term care hospitals and hospital-based providers (inpatient rehabilitation, skilled nursing and home health) where relevant.